
Ending the COVID-19 pandemic relies largely on the uptake of COVID-19 vaccines, with the goal of reaching herd immunity. As of 23 June 2021, 2.75 billion doses of COVID-19 vaccinations had been administered, and 791 million people were fully vaccinated, representing 10.1% of the world’s population.1 And yet, despite the threat of ongoing lockdowns, death, illness (both physical and mental), serious impacts on people’s lives and the global economy, the ‘anti-vax’ movement is stronger than ever.
Vaccine hesitancy is not new. We in the public health space have been fighting fear and hysteria with evidence since at least 1998, when Andrew Wakefield and colleagues published a (now infamous and completely debunked) series in the Lancet that linked the MMR vaccine to behavioural regression and pervasive developmental disorder in children.2 Even before the initial COVID-19 outbreak occurred in late 2019, the WHO had labelled vaccine hesitancy as one of the top 10 threats to global public health.
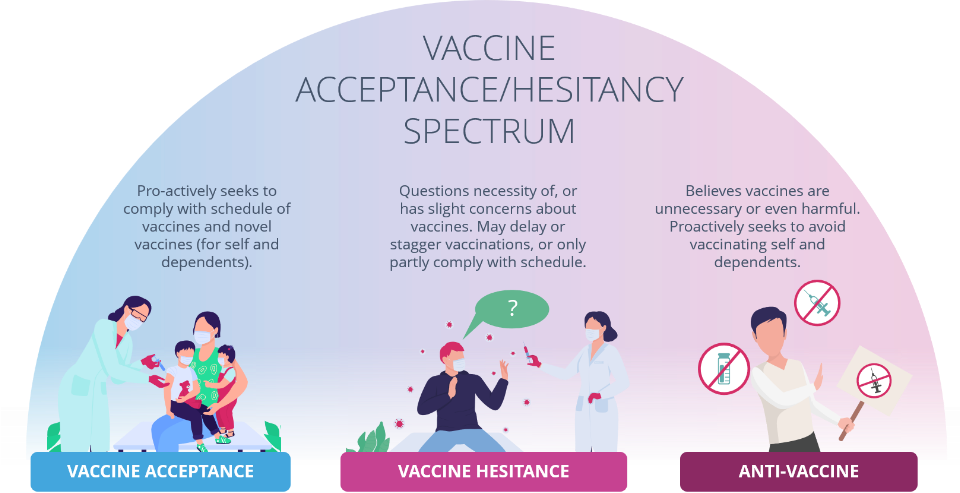
Vaccine hesitancy exists on a spectrum. It includes those who delay getting vaccines, only accept some vaccines or refuse all vaccines (‘known as anti-vaxxers’). Our challenge, as public health specialists, is not to force vaccination, but to help shift all people on the vaccine hesitancy spectrum closer towards vaccine acceptance, so that they can make evidence-informed decisions to vaccinate themselves and their children, knowing in their hearts and minds that they are doing the right thing and the safe thing for themselves, their loved ones, and the broader community.
Though many in society marvelled at and celebrated the speed with which new vaccine technologies (especially mRNA) were developed, tested, approved and distributed, others doubted the thoroughness and veracity of the review process, and an entirely new sub-group of conspiracy theorists (known as ‘COVID-deniers’) evolved. Among their claims is that a group of elites created and are using COVID-19 and its vaccine to make a profit and control people.3 As absurd as some of these claims may seem, the risk posed to population health is real. In this way, COVID-19 has added significant fuel to the vaccine hesitancy fire, and whilst we have seen a few notable anti-vaxxer’s become acceptors of the COVID-19 vaccine4, we have seen more people who are vaccine acceptors when it comes to the routine immunization schedule finding common ground with anti-vaxxers.
This, along with COVID-related interruptions and lags in vaccine schedules, has the potential to undo decades of action towards eliminating vaccine-preventable illnesses, including many communicable (e.g., diphtheria) and non-communicable diseases (e.g., cervical cancer, for which 91% of cases are caused by HPV).5 6
How can policy efforts and the life sciences industry help to improve vaccine acceptance and reduce vaccine hesitancy?
In 2011, the World Health Organization’s (WHO) Strategic Advisory Group of Experts (SAGE) on Immunization noted the impact of ‘reluctance to accept immunization’ on the uptake of vaccines in both developed and developing countries, and established a working group (WG) on vaccine hesitancy in response. The SAGE WG acknowledges that vaccine hesitancy is a complex issue, and no single strategy can address it. While Oxford academics have presented arguments for mandatory vaccinations and even payment for novel vaccines,7 the WHO shies away from policies that mandate an action or behaviour because such policies “interfere with individual liberty and autonomy.” Instead, the WHO states “it is better to work on information campaigns and making vaccines accessible”.8
The SAGE WG’s 2014 Review of Strategies to Address Vaccine Hesitancy found that there are 1) few existing strategies that have been explicitly designed to address vaccine hesitancy, and 2) even fewer strategies that have been evaluated for impact. They also found that interventions are often only half-conceived, target audiences are not always appropriately identified, and there is a lack of rigorous understanding of the actual problem.9
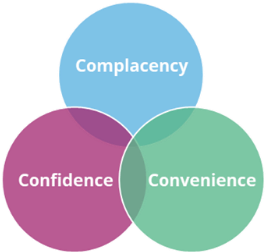
Historically (or at least the post-Wakefield/pre-COVID era spanning 1998-2018), the three main drivers of ‘reluctance to accept immunization’ were: lack of confidence, complacency, and lack of convenience. Right now, the key reasons for vaccine hesitancy stem from fear, disinformation, distrust, and defiance in the face of mandatory vaccine campaigns. Therefore, our policy responses need to address both pre- and post-COVID drivers.
How can policy help to address these deep-rooted beliefs and misconceptions in time to avert unnecessarily protracted or recurrent waves of COVID-19 and vaccine preventable illnesses (VPI) more broadly?
This is not about policy responses that simply “get the job done”, rather, it is about policies that, by their very nature, improve vaccine acceptance.
Policy-related and other (e.g., communications-based, etc.) solutions to address vaccine hesitancy must seek to address the root cause and not merely the symptoms, which makes this task almighty but not insurmountable. The following table summarises some key drivers of vaccine hesitancy, possible root causes, and potential efforts that the life sciences industry can implement to address the root causes. Most of them address ‘big picture’ issues in policy, including transparency, trust, decision making processes, and accountability.
Drivers of vaccine hesitancy (‘symptoms’)
Confidence in vaccines (including fear, disinformation, and distrust)
Possible root cause of drivers
- Distrust in ‘Big Government’ and key global stakeholders (including the UN, etc.).
- Distrust in ‘Big Pharma’.
- Distrust of medical establishments, due to systemic racism or past misuse.
- Concerns about vaccine efficacy and side effects.
- Difficulty in conveying complex scientific findings and decision-making processes to the lay public.
- Perceived lack of accountability measures in the event of unacceptably high rates of Adverse Events following Immunization (AEFIs).
- Lack of accountability measures in the event of cronyism relating to government contracts.
- Difficulty in identifying and removing disinformation from circulating, especially online.
- Difficulty in identifying trusty sources, and differentiating fake news from real news (among both those who report the news, and those who consume it)
Potential efforts that the life sciences industry can implement to address the root causes:
- Acknowledge that cronyism and corruption in all its forms undermine public health, go against social values, and damage the reputation of both governments and entire industries. Become vocal advocates for its elimination, and for enforceable accountability measures if/when it does occur.
- Adopt a policy of addressing disinformation head-on. Collaborate with tech companies like Twitter, Google, and Facebook to address fake news and ensure the public can easily find accurate information.
- Publisha details of the veracity of regulatory processes, and regulatory agencies’ commitment to handling and communicating issues if/as they arise.
- Publisha the principles and processes that guide government decisions and actions in vaccine procurement, distribution, prioritisation, and administration.
- Allow representatives from reputable and appropriate civil society or professional organizations (e.g., Royal Colleges and medical societies) to audit meetings between governments and industry where ‘big decisions’ are made, and to review terms of contracts awarded.
- Publisha a detailed explanation of AEFIs.
a targeting different population groups, in different settings, including on social media, using lay terms
Complacency
Possible root cause of drivers
- Privilege (being able to afford quality medical care/time off work, etc., in the event of illness).
- Perception that they are unlikely to contract the VPI or be significantly impacted by it.
- Naivety and/or proximity from the risk (e.g., having never seen anyone with polio, or known anyone who has had COVID-19).
Potential efforts that the life sciences industry can implement to address the root causes:
- Engage representatives from different population target groups when developing vaccination strategies to genuinely listen to and understand their motivators and hesitations and to inform key communications.
- Develop powerful, positive (not fear-based), informative and emotive public health awareness campaigns that educate the lay public about the benefits to individuals, families, vulnerable populations, and all of society, from achieving and maintaining high vaccine coverage rates.
- Explaina why high vaccination rates are necessary in all settings and at all levels (low-, middle- and high-income countries, and in every region of every country).
a targeting different population groups, in different settings, including on social media, using lay terms
Convenience
Possible root cause of drivers
- Highly centralized health system structures that position vaccine delivery services in traditional healthcare settings.
- Indirect costs associated with vaccination (time off work for vaccination and recovery from side-effects, transport costs, etc.).
- Inequitable distribution of vaccines to high income countries or urban areas.
Potential efforts that the life sciences industry can implement to address the root causes:
- Advocate for and invest in infrastructure (mobile units, etc.) that helps to deliver vaccines ‘where people are’ in the community (schools, workplaces, marketplaces, in rural and remote settings, etc.).
- Advocate for policies that support paid time off for vaccination and recovery, especially for key workers and vulnerable populations.
- Commit to donating a percentage of vaccines to support coverage in hard-to-access locations.
- Commit to supporting infrastructure and operationalization of vaccines in hard to access locations
- Innovate to reduce cold chain complexities (i.e., stability at higher temperatures or longer storage life)
- Develop meaningful partnerships, joint efforts, and collaborations to create important vaccine infrastructure.
Defiance
Possible root cause of drivers
- Lack of ability to differentiate between ‘anti-vax propaganda’ and real evidence.
- Epistemic reasons10 – a ‘search for the reasons why’ and the consumption of, interaction with, and sharing of disinformation on the internet.
- Existential reasons7 – seeking to feel and exercise autonomy over what happens to you.
- Social motives7– a sense of belonging to a group that has access to or understands a ‘truth’ that the rest of society is not privy to and is therefore superior to ‘the sheep’ (vaccine acceptors).
Potential efforts that the life sciences industry can implement to address the root causes:
- Engage social influencers (including influencers who may be on the vaccine hesitancy spectrum) to understand whether their views are rooted in epistemic, existential or social motives.
- Develop engagement platform and education programmes with appropriate messaging to openly and attentively listen to and address the concerns of people who are vaccine hesitant.
How can Policy Wisdom support these efforts?

We are perfectly positioned as a neutral bridge to connect industry, government, civil society and patient groups. We help all sides to listen better, respond more effectively, and act in the best interests of public health.

We are passionate public health experts who specialize in communications and policy. We can help you tell your side of the story in a way that different stakeholders will understand and respect.

We are results-oriented and can help you shift from wanting to be a better partner in public health to being a true partner in public health.
References:
1 Our World in Data. (2021). Statistics and Research: Coronavirus (COVID-19) Vaccinations. Last updated 23 June, 2021. Accessed 14 June 2021, from: https://ourworldindata.org/covid-vaccinations
2 Rao, TS. And Andrade, C. (2011). The MMR Vaccine: vaccine and autism: Sensation, refutation and Fraud.” Indian journal of psychiatry. Vol 53(2), 95-96. Accessed 23 June, 2021., from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3136032/
3 Shepherd, T. (2020). ‘It’s psychologically easier’: how anti-vaxxers capitalised on coronavirus fears to spread misinformation. The Guardian. Accessed 14 June 2021, from:https://www.theguardian.com/society/2020/jun/06/its-psychologically-easier-how-anti-vaxxers-capitalised-on-coronavirus-fears-to-spread-misinformation
4 Haelle, T. (2021) Why a Former Anti-Vax Influencer Got Her COVID-19 Shot. Accessed 23 June, 2021., from: https://www.texasmonthly.com/news-politics/anti-vax-influencer-covid-19-vaccine-hesitancy/
5 Aquino, M. (2020). Peru reports first diphtheria case in 20 years amid low vaccination rate. Accessed 23 June, 2021., from: https://www.reuters.com/article/us-health-coronavirus-bolivia-diptheria-idUSKBN27D267
6 CDC. 2020. How Many Cancers Are Linked with HPV Each Year?. Accessed 23 June, 2021., from: https://www.cdc.gov/cancer/hpv/statistics/cases.htm
7 Savulescu, J. (2021). Good reasons to vaccinate: mandatory or payment for risk? Journal of Medical Ethics 2021;47:78-85. https://jme.bmj.com/content/47/2/78.info
8 World Health Organization. COVID-19 virtual press conference 7 December 2020. Accessed 14 June 2021, from: https://www.who.int/publications/m/item/covid-19-virtual-press-conference-transcript—7-december-2020
9 WHO SAGE working group dealing with vaccine hesitancy. (2014). Strategies For Addressing Vaccine Hesitancy – A Systematic Review. Accessed 23 June, 2021, from: https://www.who.int/immunization/sage/meetings/2014/october/3_SAGE_WG_Strategies_addressing_vaccine_hesitancy_2014.pdf
10 Douglas, K. (2021). Speaking of Psychology: Why people believe in conspiracy theories. American Psychological Association. Accessed 14 June 2021, from: https://www.apa.org/research/action/speaking-of-psychology/conspiracy-theories